During the time course of an athlete’s career there is a high risk of suffering a significant knee or lower limb injury during sports participation. Over the past four years, the cornerstone of my research has been looking at anterior cruciate ligament (ACL) and hamstring strain injuries (HSI) in sport. Many of you may be thinking, “what’s the big deal?”, but what if I told you, that in Australia, ACL injuries cost professional sporting organisations an estimated AUD$17 000 – 25 000 per athlete for surgery and rehabilitation (2, 3), while HSIs cost sport organisations millions of dollars (4, 5).
Understanding lower limb injury
Both ACL and hamstring injuries are major problems in sport and despite some progress in the development of injury prevention and rehabilitation practices, the incidence and recurrence rates of each are still high. Together, hamstring strain and ACL injuries comprise the injuries with the highest incidence (most common) and prevalence (most severe) in sport, respectively (6) (Figure 1). Although, recent trends in elite male professional football suggest that ACL (7) and hamstring injury rates (8) are not declining. However, results may vary in different sports and at different levels of competition.
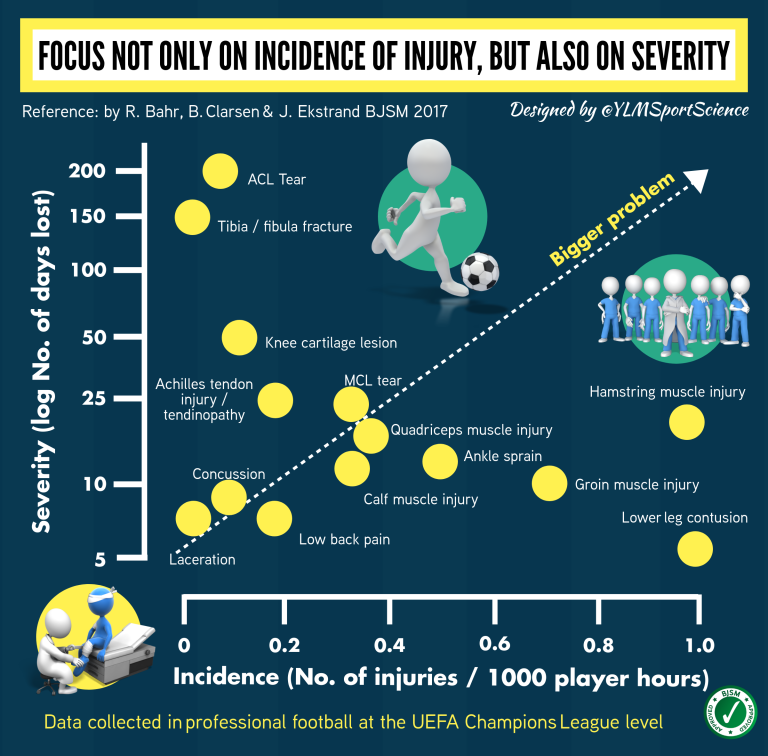
Figure 1. Incidence and severity of injuries in the UEFA Champions League (6).
The hamstring muscle complex
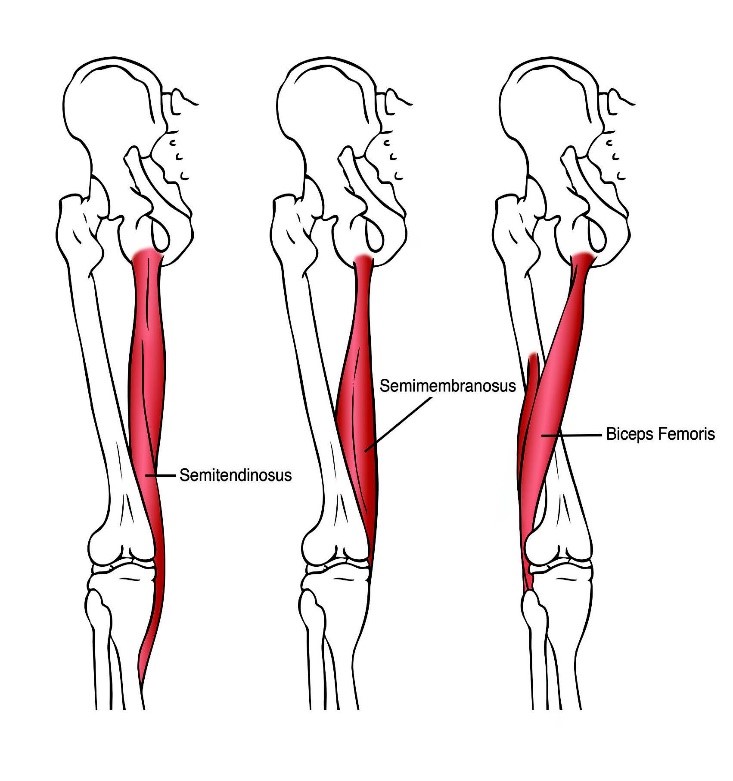
Figure 2. The hamstring muscle complex.
The hamstring muscle complex describes a group of three muscles located on the posterior thigh – semitendinosus, semimembranosus, and biceps femoris; which is further divided into a long and a short head (9) (Figure 2). With the exclusion of biceps femoris short head, the hamstrings are biarticular muscles because they cross both the posterior aspects of the hip and knee joints (10), which allow the long hamstrings to perform flexion at the knee and extension of the hip during concentric contraction. Collectively, the hamstrings’ common actions are hip extensors and knee flexors; however, each muscle exhibits significant differences in morphology (e.g., physiological cross sectional area), architecture (e.g., fascicle length and pennation angles) and function (e.g., activation patterns) (9, 11). Hamstring muscles play important roles in running and side-cutting movements which are sometimes associated with hamstring strain and ACL injuries (12, 13). Eccentric strength training for the hamstrings plays an important role in reducing strain injuries to those muscles (14-16) and the knee flexors are also the primary form of muscular support for the ACL, acting to stabilise the knee and prevent excessive anterior tibial translation (17-19). Consequently, strengthening the knee flexors is considered an important component of ACL (19, 20) and hamstring injury prevention practices (15, 16, 21).
MECHANISMS(S) OF HAMSTRING STRAIN AND ACL INJURIES
HSIs usually involve damage to the muscle tendon unit and are thought to be caused by forceful eccentric contraction or from an excessive stretch of the muscle tendon unit (22). The proposed mechanisms for HSIs include kicking, tackling, cutting, stooping while running and excessive stretching (23-26). Though, the majority of HSIs in running based sports occur during high-speed activities (25-29). During eccentric contractions at medium to long muscle lengths, there are moderate to high levels of muscle strain (muscle length) (30). Strong eccentric actions also expose muscle-tendon units to high degrees of muscle stress, measured as force per unit of cross-sectional area (30).
Most ACL tears are non-contact injuries that occur during landing, changes of direction or deceleration while hip adduction, internal femoral rotation, external tibial rotation and knee valgus is often identifiable at the time of injury (31, 32). ACL reconstructions are almost always considered essential for restoring adequate knee joint stability (33, 34), and they usually involve one of two autogenous grafts harvested from either the ipsilateral semitendinosus and gracilis or the patella tendon (35-37). However, the semitendinosus muscle provides support to the ACL by resisting external tibial rotation and anterior tibial translation (38, 39), and the impact of semitendinosus tendon grafts on the long term function of this muscle is unclear (40).
A PREVIOUS LOWER LIMB INJURY IS THE BIGGEST RISK FACTOR FOR A SUBSEQUENT INJURY IN THE FUTURE
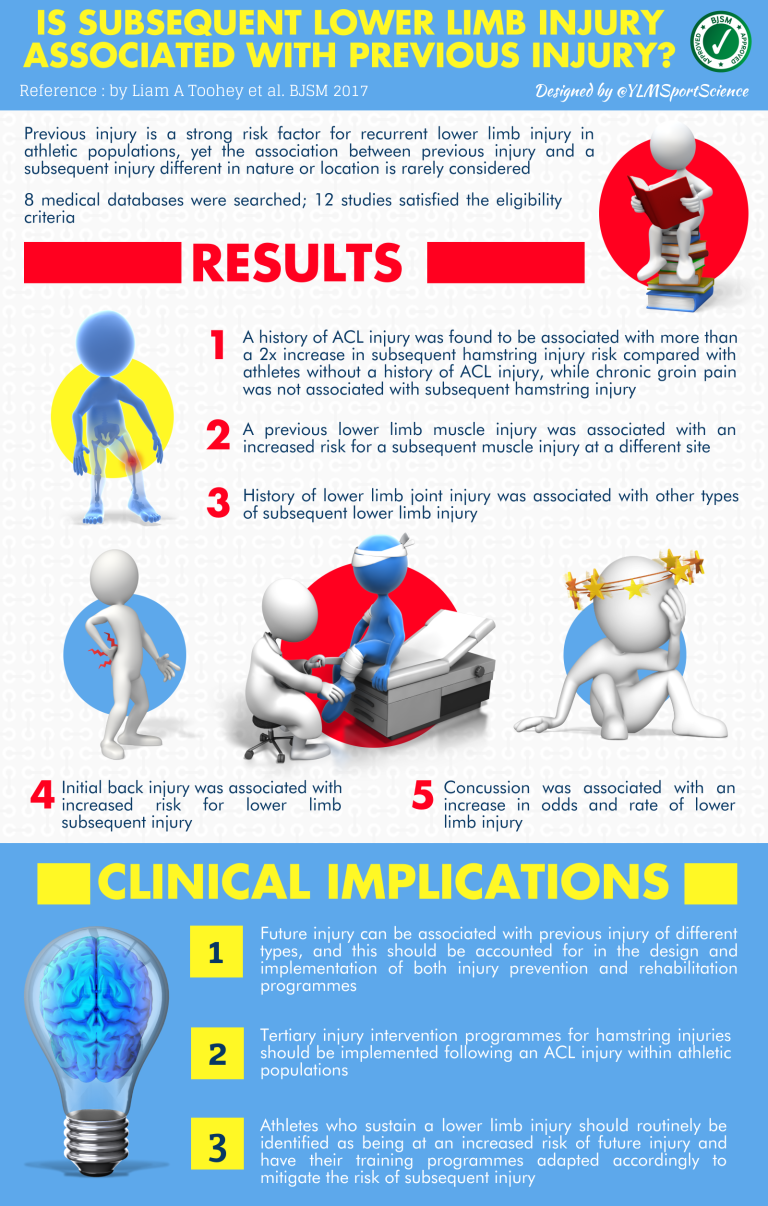
Figure 3. Previous lower limb injury and risk of subsequent injury (1).
A history of HSI is a very strong predictor of future HSI (41-44). One prospective study in elite soccer players has shown that players who suffered a HSI in the previous season were 11.6 times more likely to sustain a recurrent HSI in the subsequent season (45). The mechanism(s) increasing the risk of future HSI in individuals with a history of this injury remain unclear; however, it is likely to occur from the contribution of a number of maladaptation’s following HSI (46, 47) or the persistence of risk factors that contributed to the initial injury (48-50). Meanwhile, a history of ACL injury is also associated with an increased risk of a new knee injury (51, 52). A history of ACL injury is a strong risk factor for subsequent re-injury and this is due to many factors, including; sub-optimal surgery, muscular weakness and imbalances, weakening of ligaments, altered kinematics and diminished proprioception after initial injury (53-55). A history of ACL injury results in deficits in proprioception and range of motion which may alter the coordination of previously learnt movements (56, 57). Therefore, it is possible that the common hamstring graft reconstruction technique leaves athletes more prone to hamstring strain injury. The biomechanical changes that occur after ACL injury (41, 58) and hamstring muscle weakness (59) are thought to contribute to the increased risk of future hamstring injury after ACL reconstruction and rehabilitation.
KEY TAKE HOME MESSAGES:
- A prior ACL injury is the strongest predictor of future hamstring strain injury, followed by a recent (12 month) history of hamstring strain injury.
- Athletes who undergo an ACL reconstruction (irrespective of graft technique) have an augmented risk of future hamstring strain injury if they have also suffered a recent (12 month) history of hamstring strain injury.
- ACL rehabilitation programs need to be improved given athletes are at significantly elevated risk of hamstring strain injury despite successfully returning to sport, often with ~12 months of rehabilitation.
By Daniel Messer.
Anyone who would like to know more information regarding exercise selection in ACL and hamstring injury prevention and rehabilitation programs should contact Daniel.
References
- Toohey LA, Drew MK, Cook JL, Finch CF, Gaida JE. Is subsequent lower limb injury associated with previous injury? A systematic review and meta-analysis. Br J Sports Med. 2017;51(23):1670-8.
- Orchard J, Seward H, McGivern J, Hood S. Rainfall, evaporation and the risk of non-contact anterior cruciate ligament injury in the Australian Football League. Med J Aust. 1999;170(7):304-6.
- Orchard J, Seward H, McGivern J, Hood S. Intrinsic and extrinsic risk factors for anterior cruciate ligament injury in Australian footballers. Am J Sports Med. 2001;29(2):196-200.
- Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit of injuries in professional football-analysis of preseason injuries. Br J Sports Med. 2002;36(6):436-41; discussion 41.
- Verrall GM, Kalairajah Y, Slavotinek JP, Spriggins AJ. Assessment of player performance following return to sport after hamstring muscle strain injury. J Sci Med Sport. 2006;9(1-2):87-90.
- Bahr R, Clarsen B, Ekstrand J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 2017.
- Walden M, Hagglund M, Magnusson H, Ekstrand J. ACL injuries in men’s professional football: a 15-year prospective study on time trends and return-to-play rates reveals only 65% of players still play at the top level 3 years after ACL rupture. Br J Sports Med. 2016;50(12):744-50.
- Ekstrand J, Walden M, Hagglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med. 2016;50(12):731-7.
- Woodley SJ, Mercer SR. Hamstring muscles: architecture and innervation. Cells Tissues Organs. 2005;179(3):125-41.
- Koulouris G, Connell D. Hamstring muscle complex: an imaging review. Radiographics. 2005;25(3):571-86.
- Markee JE, Logue JT, Jr., Williams M, Stanton WB, Wrenn RN, Walker LB. Two-joint muscles of the thigh. J Bone Joint Surg Am. 1955;37-A(1):125-42.
- Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226-32.
- Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. Am J Sports Med. 2006;34(2):299-311.
- Mjolsnes R, Arnason A, Osthagen T, Raastad T, Bahr R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand J Med Sci Sports. 2004;14(5):311-7.
- Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18(1):40-8.
- van der Horst N, Smits DW, Petersen J, Goedhart EA, Backx FJ. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43(6):1316-23.
- Kingma I, Aalbersberg S, van Dieen JH. Are hamstrings activated to counteract shear forces during isometric knee extension efforts in healthy subjects? J Electromyogr Kinesiol. 2004;14(3):307-15.
- Hiemstra LA, Webber S, MacDonald PB, Kriellaars DJ. Knee strength deficits after hamstring tendon and patellar tendon anterior cruciate ligament reconstruction. Med Sci Sports Exerc. 2000;32(8):1472-9.
- Silvers HJ, Mandelbaum BR. Prevention of anterior cruciate ligament injury in the female athlete. Br J Sports Med. 2007;41 Suppl 1(suppl 1):i52-9.
- Boden BP, Griffin LY, Garrett WE, Jr. Etiology and Prevention of Noncontact ACL Injury. Phys Sportsmed. 2000;28(4):53-60.
- Petersen J, Thorborg K, Nielsen MB, Budtz-Jorgensen E, Holmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39(11):2296-303.
- Agre JC. Hamstring injuries. Proposed aetiological factors, prevention, and treatment. Sports medicine (Auckland, NZ). 1985;2(1):21-33.
- Verrall GM, Slavotinek JP, Barnes PG, Fon GT. Diagnostic and prognostic value of clinical findings in 83 athletes with posterior thigh injury: comparison of clinical findings with magnetic resonance imaging documentation of hamstring muscle strain. Am J Sports Med. 2003;31(6):969-73.
- Ekstrand J, Gillquist J. Soccer injuries and their mechanisms: a prospective study. Med Sci Sports Exerc. 1983;15(3):267-70.
- Woods C, Hawkins RD, Maltby S, Hulse M, Thomas A, Hodson A, et al. The Football Association Medical Research Programme: an audit of injuries in professional football–analysis of hamstring injuries. Br J Sports Med. 2004;38(1):36-41.
- Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34(8):1297-306.
- Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50(24):1524-35.
- Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in Australian footballers. Med Sci Sports Exerc. 2015;47(4):857-65.
- Bourne MN, Opar DA, Williams MD, Shield AJ. Eccentric Knee Flexor Strength and Risk of Hamstring Injuries in Rugby Union: A Prospective Study. Am J Sports Med. 2015;43(11):2663-70.
- Garrett WE, Jr. Muscle strain injuries: clinical and basic aspects. Med Sci Sports Exerc. 1990;22(4):436-43.
- Besier TF, Lloyd DG, Ackland TR. Muscle activation strategies at the knee during running and cutting maneuvers. Med Sci Sports Exerc. 2003;35(1):119-27.
- Cochrane JL, Lloyd DG, Buttfield A, Seward H, McGivern J. Characteristics of anterior cruciate ligament injuries in Australian football. J Sci Med Sport. 2007;10(2):96-104.
- Liow RY, McNicholas MJ, Keating JF, Nutton RW. Ligament repair and reconstruction in traumatic dislocation of the knee. J Bone Joint Surg Br. 2003;85(6):845-51.
- Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45(7):596-606.
- Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38(10):1968-78.
- Pinczewski LA, Lyman J, Salmon LJ, Russell VJ, Roe J, Linklater J. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med. 2007;35(4):564-74.
- Ardern CL, Webster KE, Taylor NF, Feller JA. Hamstring strength recovery after hamstring tendon harvest for anterior cruciate ligament reconstruction: a comparison between graft types. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2010;26(4):462-9.
- Nomura Y, Kuramochi R, Fukubayashi T. Evaluation of hamstring muscle strength and morphology after anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 2015;25(3):301-7.
- Ejerhed L, Kartus J, Sernert N, Kohler K, Karlsson J. Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med. 2003;31(1):19-25.
- Burks RT, Crim J, Fink BP, Boylan DN, Greis PE. The effects of semitendinosus and gracilis harvest in anterior cruciate ligament reconstruction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005;21(10):1177-85.
- Verrall GM, Slavotinek JP, Barnes PG, Fon GT, Spriggins AJ. Clinical risk factors for hamstring muscle strain injury: a prospective study with correlation of injury by magnetic resonance imaging. Br J Sports Med. 2001;35(6):435-9; discussion 40.
- Orchard JW. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am J Sports Med. 2001;29(3):300-3.
- Gabbe BJ, Bennell KL, Finch CF, Wajswelner H, Orchard JW. Predictors of hamstring injury at the elite level of Australian football. Scand J Med Sci Sports. 2006;16(1):7-13.
- Hagglund M, Walden M, Ekstrand J. Previous injury as a risk factor for injury in elite football: a prospective study over two consecutive seasons. Br J Sports Med. 2006;40(9):767-72.
- Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med. 2004;32(1 Suppl):5S-16S.
- Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports medicine (Auckland, NZ). 2012;42(3):209-26.
- Fyfe JJ, Opar DA, Williams MD, Shield AJ. The role of neuromuscular inhibition in hamstring strain injury recurrence. J Electromyogr Kinesiol. 2013;23(3):523-30.
- Silder A, Heiderscheit BC, Thelen DG, Enright T, Tuite MJ. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skeletal Radiol. 2008;37(12):1101-9.
- Witvrouw E, Danneels L, Asselman P, D’Have T, Cambier D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players – A prospective study. Am J Sports Med. 2003;31(1):41-6.
- Croisier JL, Forthomme B, Namurois MH, Vanderthommen M, Crielaard JM. Hamstring muscle strain recurrence and strength performance disorders. Am J Sports Med. 2002;30(2):199-203.
- Faude O, Junge A, Kindermann W, Dvorak J. Risk factors for injuries in elite female soccer players. Br J Sports Med. 2006;40(9):785-90.
- Walden M, Hagglund M, Ekstrand J. High risk of new knee injury in elite footballers with previous anterior cruciate ligament injury. Br J Sports Med. 2006;40(2):158-62; discussion -62.
- Hewett TE, Di Stasi SL, Myer GD. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(1):216-24.
- Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27(6):699-706.
- Murphy DF, Connolly DA, Beynnon BD. Risk factors for lower extremity injury: a review of the literature. Br J Sports Med. 2003;37(1):13-29.
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin J Sport Med. 2012;22(2):116-21.
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. Am J Sports Med. 2014;42(7):1567-73.
- Koulouris G, Connell DA, Brukner P, Schneider-Kolsky M. Magnetic resonance imaging parameters for assessing risk of recurrent hamstring injuries in elite athletes. Am J Sports Med. 2007;35(9):1500-6.
- Mohtadi N, Barber R, Chan D, Paolucci EO. Complications and Adverse Events of a Randomized Clinical Trial Comparing 3 Graft Types for ACL Reconstruction. Clin J Sport Med. 2016;26(3):182-9.